
Sign In to Your Account
Subscribers have complete access to the archive.
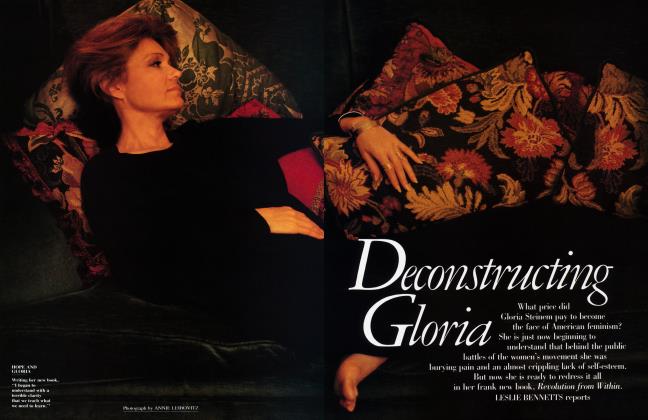
Sign In Not a Subscriber?Join NowSins of the Fathers
Psychoanalyst ALICE MILLER explores the silent trauma of the invaded child
“One of the laws governing a child’s existence is determined by what parents need from their child, and sexuality is no exception here’’
THE effects of the abuse of power X can easily be identified in the childhood of every patient in therapy. But sexual abuse is still the most difficult to uncover—and we know it is the fact of concealment that isolates the child, leaving him alone with his secret and making him ill. The young Sigmund Freud had already discovered and described this tragedy in 1896; unfortunately, it was almost impossible for Freud to stand by his findings in a society in which the child, never the parent, was to be blamed for any moral transgression. Freud would later claim that the incidents of sexual abuse in childhood reported by his patients hadn’t actually happened, that they were fantasies resulting from the child’s own sexual drives. This “parent-protecting” outlook (known as the “drive” theory and centering upon Freud’s hypotheses of infantile sexuality and the Oedipus complex) has been taught ever since, as far as I know, in all psychoanalytic institutes. Of course, Freud’s original “seduction” theory, with its assumption that every neurosis comes from sexual rape in childhood, was obviously wrong and had to be abandoned. There are countless ways in which children can be mistreated, and the narcissistic significance of the abuse of power is being increasingly recognized. Nevertheless, if patients are to be helped, sexual traumatization must not be discounted or denied—as many therapists have been inclined to do, thanks to the drive theory.
Every religion has its taboos, which must be accepted by its followers if they do not want to be rejected by the community of believers. But what happens when a great scientific discovery, relevant for everyone, is made the exclusive property of one school of thought and is surrounded by dogmas and taboos? A paradoxical situation then arises in which the original discovery, which might have been the starting point for further findings and for a substantial heightening of consciousness, stagnates because the dogmas that have become entrenched in the meantime would be threatened by new findings.
What I have observed about “infantile sexuality” in the analyses I have conducted myself and in those I have supervised does not confirm the validity of the drive theory.
Some, though by no means all, of the anxiety, bewilderment, and uncertainty present in every patient’s childhood is of a sexual nature. But I now no longer interpret such difficulties as a defense against the child’s own sexual desire but in part as reactions to adults’ sexual desires (conscious or unconscious), of which the child is the object. The child will make every attempt to satisfy the adult’s desires or at least not to frustrate them to any great extent, even producing pseudosexual feelings, because he needs tenderness at any cost and cannot run the risk of rejection. One of the inescapable laws governing a child’s existence is determined by what parents need from their child, and sexuality is no exception here.
In all of psychoanalytic theory there is very rarely any mention of the effect a child has on sexually unfulfilled parents. Furthermore, the question is rarely raised of what it means for little children, during a display of affection, to see in their mother’s or father’s eyes a sexual need they would like to respond to but can’t. Encountering this look alone causes only a very mild form of disorientation, but a whole gamut of incomprehensible and frightening sexual contacts between child and adult—up to and including rape—occurs much more frequently than people like to admit.
It is quite natural for children to awaken sexual desire in the adult because they tend to be beautiful, cuddly, affectionate, and because they admire the adult so much, probably more than anyone else does. If adults have a satisfying sex life with another adult, they will have no need either to act upon the desires aroused by the child or strive to ward them off. But if they feel themselves humiliated and not taken seriously by their partner, if their own needs were never allowed to unfold or mature, or if they were themselves seduced and violated as children, then these adults will show a strong tendency to impose their sexual needs on the child. Unfortunately, many adults are convinced that what happens to very little children has no consequences at all and will never be divulged to a third party.
It has been my experience that a therapist makes much greater therapeutic progress if he or she tries to understand patients’ sexual problems as a result of sexual abuse by adults rather than in terms of infantile sexuality. I do not interpret the seductive behavior of a socalled hysterical patient as an expression of sexual desires but as an unconscious message concerning an event the patient has completely forgotten, which can be approached only by way of this reenactment. I believe that in an active role the patient will repeatedly demonstrate what once—or more than once— happened to her or him but which the patient cannot remember because it was too traumatic to retain on a conscious level without the aid of an empathic support figure. Instead, the patient reenacts the unconscious trauma of childhood that caused the illness.
WHEN I speak of unconscious W trauma, I do not mean that one specific event will inevitably cause neurosis but rather the entire atmosphere of early childhood, which comes to light in the transference and countertransference between patient and analyst. It is not necessarily emotional deprivation that so often leads to psychic disturbances but it is above all narcissistic wounds— including sexual abuse. These wounds occur at that time of life when the child is most helpless and are concealed by subsequent repression. While this repression ensures that the parents’ secret will be safe, the child’s lack of conscious knowledge blocks access to his or her feelings and vitality. Not being able to talk about or even know about these wounds is what later leads to pathological developments.
Virginia Woolf, who suffered from repeated psychotic episodes from the time she was thirteen, committed suicide at the age of fifty-nine. Her biographer, Quentin Bell, reports that she suffered from “a cancer of the mind, a corruption of the spirit” and heard ‘‘the voices of insanity.” He writes: ‘‘I do not know enough about Virginia’s mental illnesses to say whether [her] adolescent trauma was in any way connected with them.” Yet on the preceding page he tells in detail about the way the two little girls, Virginia and her sister Vanessa, were used for years by their much older half-brother George for his sexual ‘‘skirmishes.” Not without empathy Bell says:
To the sisters it simply appeared that their loving brother was transformed before their eyes into a monster, a tyrant against whom they had no defence, for how could they speak out or take any action against a treachery so covert that it was half unknown even to the traitor? Trained as they were to preserve a condition of ignorant purity they must at first have been unaware that affection was turning to concupiscence, and were warned only by their growing sense of disgust. To this, and to their intense shyness, we may ascribe Vanessa’s and Virginia’s long reticence on the subject. George was always demonstratively emotional, lavish and irresponsible in his endearments and his embraces; it would have taken a very knowing eye to perceive that his caresses went perhaps further than was proper in even the most loving of brothers, and the bedtime pettings may have seemed no more than a normal extension of his daytime devotion. It would have been hard for his half-sisters to know at what point to draw a line, to voice objections, to risk evoking a painful and embarrassing scandal: harder still to find someone to whom they could speak at all.
These sexual games continued over a number of years until Virginia was eleven. In her ‘‘loving” environment, there was not a soul in whom Virginia could have confided without having to fear that she herself would be blamed. Perhaps she could have overcome her hesitancy if another half-brother had not already done something similar when she was six. In a letter to Ethel Smyth dated January 12, 1941 (the year of Woolf’s suicide!), Virginia writes: “I still shiver with shame at the memory of my half-brother, standing me on a ledge, aged about 6 or so, exploring my private parts.” A document that was discovered later revealed that the halfbrother referred to here was not George but Gerald. Although Woolf’s biographer reports that she ‘‘felt that George had spoilt her life before it had fairly begun,” the link between these events and her mysterious psychosis remains a riddle to him.
It has been my experience that in the late stages of a patient’s analysis, memories often come to the surface of being fondled as a child by an uncle or a stranger. The patient did not dare to resist these advances or even tell anyone what had happened. From the perspective of Freud’s drive theory the obvious thing to do would be to sound the patient out about the pleasurable feelings supposedly experienced at the time. Patients often accept this approach without resistance because they are so used to not being understood. Yet it is apparent from the foregoing how completely such interpretations can ignore the child’s very real distress and loneliness. It also frequently turns out that the remembered ‘‘uncle” was a screen memory. Only when this experience has been relived and given empathic attention by the analyst can the even earlier repressed memory of a similar experience with the father or older brother emerge. The recollection is often accompanied by numerous dreams with similar content and by new dynamics in the transference between patient and analyst. Again and again in the transference and in relationships with presentday partners, the need then arises to have privacy, one’s own carefully guarded space (A Room of One’s Own), to stop letting oneself be used in all possible kinds of ways, to be able to say no, to experience oneself as a sepaEate person. Suspicion also emerges of the other person’s intentions, combined with a great fear of losing the loved person if one doesn’t place oneself entirely at the other’s disposal. During this stage of analysis, patients often dream, for example, that for the first time they are finally able to bring themselves to close the bathroom door. It becomes clear that they never would have dared to do this during puberty and that the father was always free to enter the bathroom whenever he pleased. One patient dreamed that he saw again the narrow passages of his earlier dreams but this time was no longer willing to squeeze through the narrow openings and bend down in order to enter the next room. Now he avoided these passages and discovered large new rooms. Another patient dreamed that she discovered a room in her apartment that could be locked securely and that belonged only to her from then on. Dreams like this have a symbolic character, for they represent freeing the self from someone else’s power, but they also bring actual early situations to light. Very often chronic insomnia or frigidity disappears at this point.
IT should be obvious that a child who -L is abused at a very early age in order to fulfill an adult’s or older sibling’s needs will be left for the rest of his life with the feeling that he had to give too much of himself. This feeling combines with a bad conscience and eventually results in the unbearable conviction that he is a bad person for always feeling exploited “without cause” and for not being glad to give away all that he has and is. The consequences of sexual abuse are not restricted to problems in one’s sexual life; they impair the development of the self and of an autonomous personality. Because anger toward the loved person cannot be expressed for fear of losing that person, ambivalence—the interlinking of love and hate—remains an important characteristic of later object relationships. The healing process begins when the once absent, repressed reactions to traumatization (such as feelings of guilt, anxiety, rage, anger, despair, pain, grief) can be articulated in therapy; only then can the symptoms disappear, whose function it had been to express the unconscious trauma in a disguised, alienated language.
Translated from the German by Hildegarde and Hunter Hannum
Subscribers have complete access to the archive.
Sign In Not a Subscriber?Join Now

